Today, I review, link to, and excerpt from Coronary microvascular disease: current concepts of pathophysiology, diagnosis and management. [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Aish Sinha,1 Haseeb Rahman,1 and Divaka Perera,1. Cardiovasc Endocrinol Metab. 2021 Mar; 10(1): 22–30. Published online 2020 Jul 16. doi: 10.1097/XCE.0000000000000223
There are 100 similar articles in PubMed.
The above article has been cited 17 times by other articles in PubMed.
All that follows is from the above resource.
Abstract
Coronary microvascular disease (CMD) is present in 30% of patients with angina and is associated with increased morbidity and mortality. We now have an improved understanding of the pathophysiology of CMD and the invasive and noninvasive tests that can be used to make the diagnosis. Recent studies have shown that management of CMD guided by physiological testing yields better results than empirical treatment. Despite major advances in diagnosing and stratifying this condition, therapeutic strategies remain limited and poorly defined. This review article discusses recent advances in understanding the pathophysiology of CMD, the modalities that are available to diagnose it clinically, current management options and a look at what is in store for the future.
Keywords: coronary microvascular disease, coronary blood flow, coronary flow reserve, microvascular resistance, nitric oxide, physiology-stratified disease endotypes
Introduction
Angina is chest pain as a result of myocardial ischaemia, and it affects up to 2 million people in the UK [1]. This has historically been viewed as the manifestation of obstructive coronary artery disease (CAD). However, up to 50% of patients with angina, who undergo elective coronary angiography, are found to have nonobstructive coronary artery disease (NOCAD) [2]. The term NOCAD encompasses a broad range of pathologies, including coronary microvascular disease (CMD), epicardial coronary artery vasospasm and enhanced cardiac nociception with disparate prognostic outlooks and therapeutic implications. Over half of all patients with NOCAD have CMD [3], which is associated with a greater risk of major adverse cardiovascular events (MACE). Several studies have demonstrated that women, presenting with angina, are more likely to suffer from NOCAD and CMD [3]. The term CMD was coined in 1988 to describe the abnormality in the microcirculation leading to an inadequate vasodilatory response, or a pathological vasoconstrictive response, to physiological or pharmacological stress [4]. The main parameter used to diagnose CMD is diminished coronary flow reserve (CFR), or impaired ability of the microvasculature to augment its blood flow in response to stress [5,6]. CFR is defined as the ratio of flow at maximal hyperaemia (usually in response to adenosine) to the flow at rest. In the context of NOCAD, CFR informs about prognosis, the presence of ischaemia and likely response to therapy [5,6]. The focus of this review article will be on the pathophysiology, diagnosis and contemporary management of CMD.
Coronary microvasculature in health
The coronary vasculature comprises of epicardial arteries (>400 µm), pre-arterioles (100–400 µm), arterioles (<100 µm) and capillaries (<10 µm). The epicardial arteries function as capacitance vessels and respond to shear forces by endothelium-mediated dilatation. Epicardial arteries are visible on coronary angiography but represent only 5–10% of the coronary vasculature. The pre-arterioles, arterioles and capillaries form the coronary microvasculature. The pre-arterioles are characterised by a measurable pressure drop along their length. The arterioles have a high resting tone and are responsible for most of the coronary vascular resistance and dilate in response to changes in myocardial oxygen demand. The capillary bed delivers oxygen and substrates to the myocytes. The coronary circulation matches myocardial oxygen demand with supply via a complex interplay between myogenic tone, metabolic signals and circulating hormones [7]. The endothelium plays an important role in the modulation of vascular tone by synthesising and releasing several vasodilator substances, such as nitric oxide (NO) [7]. Increased endothelial wall shear stress and acetylcholine are determinants of coronary blood flow (CBF) in health. Both lead to the biosynthesis of NO, which acts on the neighbouring smooth muscle cells to induce vasodilation via the NO pathway [7].
Pathophysiology of coronary microvascular disease
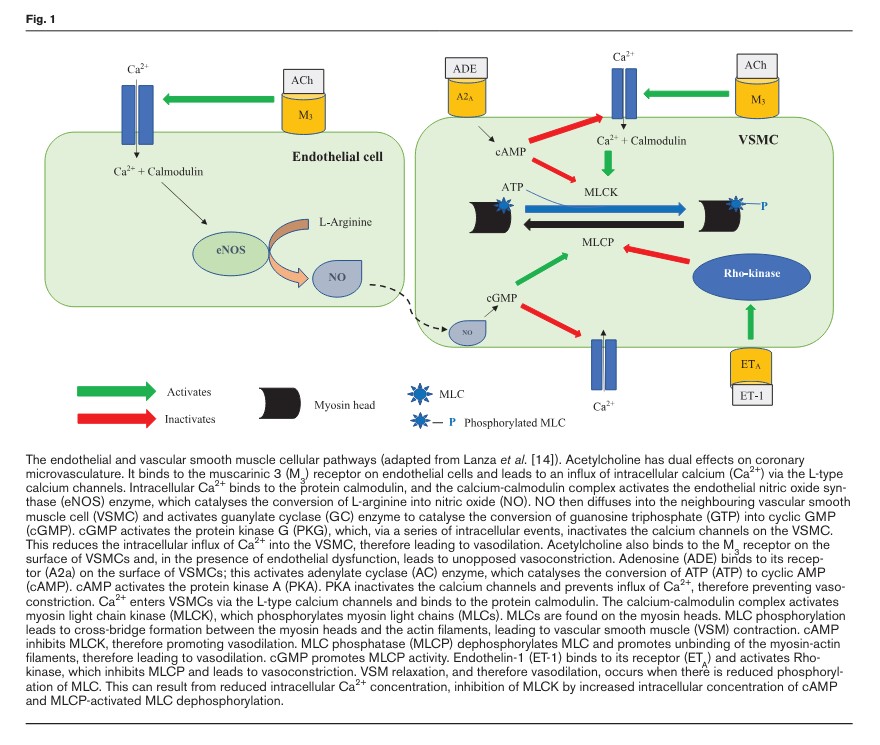
Traditionally, the pathophysiology of CMD was thought to be a combination of microvascular architectural changes and endothelial dysfunction. Microvascular architectural changes include microvascular obstruction, with luminal narrowing of the arterioles and capillaries, and capillary rarefaction [8]. Alternatively, or concurrently, endothelial or vascular smooth muscle (VSM) dysfunction may lead to an attenuated vasodilatory response or a pathological vasoconstrictive response to stimuli, leading to a blunted augmentation of, or reduction of, CBF in response to stress [9]. These cellular mechanisms are described in Fig. Fig.1.1. This can lead to a supply-demand mismatch in CBF, therefore leading to ischaemia and symptoms of angina.
This has remained the dogma of CMD pathogenesis for the past few decades. However, recent animal models and clinical physiology evaluations suggest that CMD may be a heterogeneous condition comprising distinct endotypes [5,6]. Rahman et al. have described these endotypes as ‘structural CMD’ and ‘functional CMD’ [5,6]. Both endotypes have an impaired augmentation of CBF in response to intravenous adenosine (CFR < 2.5). However, patients with structural CMD have an elevated minimal microvascular resistance (which translates to reduced maximal CBF), whereas patients with functional CMD have a normal minimal microvascular resistance, but nevertheless have reduced vasodilatory reserve as they have reduced tone at rest [5,6].
These endotypes have a similar core phenotype, with both groups demonstrating high prevalence of stress perfusion defects on cardiac magnetic resonance (CMR) imaging and reduced coronary perfusion efficiency, on wave intensity analysis, during physical exercise [5,6]. However, they differ in their pathogenesis at the microvascular level. Patients with functional CMD were found to have a heightened resting CBF [5,6]. This is suggestive of a submaximal vasodilatory state at rest, leading to an attenuated vasodilatory capacity in response to physiological stress. The elevated resting CBF in these patients could be an appropriate response to an increased myocardial oxygen demand or it could represent disordered autoregulation of the neuronal nitric oxide synthase (nNOS) pathway, which has been shown to regulate the resting CBF in both health and disease states [10,11]. On the other hand, patients with structural CMD have a normal resting CBF [5,6], similar to patients with preserved CFR, but they have an impaired ability to augment their CBF in response to physiological stress, leading to ischaemia. Patients with structural CMD appear to have more established cardiovascular risk factors, including poorly controlled hypertension, type 2 diabetes mellitus (T2DM) and a higher prevalence of exercise-induced hypertension [5,6]. It has been hypothesised that the attenuated reduction in afterload with exercise would interrupt the usual synergistic response of the coronary and peripheral circulations and predispose to ischaemia in patients with structural CMD [5,6]. However, it remains unclear whether patients with structural CMD have an impaired ability to augment their CBF as a result of architectural changes, such as microvascular hypertrophy or fibrosis limiting their ability to vasodilate, or whether it is due to dysregulation of the endothelial NOS (eNOS) pathway, which has been shown to regulate CBF in response to exertion [11].
Are functional and structural microvascular dysfunction part of a disease continuum of the coronary microvasculature? Further studies are needed to answer these pertinent mechanistic questions.
Although a detailed review of epicardial coronary artery vasospasm, and consequent vasospastic angina (VSA), is beyond the scope of this focussed review, it is worth reviewing some of the features of this condition. Vascular smooth muscle cell (VSMC) contraction is regulated by a complex system of intracellular pathways. The central molecular mechanism leading to VSMC hypercontraction is Rho kinase-mediated enhancement of myosin light chain (MLC) phosphorylation [14] (Fig. (Fig.1).1). Other mechanisms contributing towards coronary vasospasm include endothelial dysfunction, low-grade inflammation and oxidative stress. However, these are unlikely to be the primary drivers of coronary vasospasm, and likely serve as additional pathophysiological risk factors.
Clinical presentation
Angina secondary to CMD is characterised by effort-induced symptoms often indistinguishable to those observed in patients with angina triggered by obstructive CAD. Patients with CMD tend to experience prolonged episodes of chest pain and a relatively poor response to oral nitrates [15]. On the other hand, patients suffering from epicardial coronary artery vasospasm, VSA, tend to suffer from angina at rest (especially at night and early morning). These symptoms can be precipitated by hyperventilation and respond to short-acting nitrates within seconds [16].
Recently, Ong et al. have proposed the Coronary Vasomotion Disorders International Study Group criteria to diagnose CMD [17]. This diagnostic criterion includes (1) presence of symptoms of myocardial ischaemia, (2) absence of obstructive epicardial CAD, (3) evidence of objective myocardial ischaemia on functional imaging and (4) evidence of impaired coronary microvascular function. Ong et al. have suggested that the presence of four of these criteria suggests a definite diagnosis of CMD, whilst the presence of three suggests probable CMD [17]. Whilst these criteria are logical and provide a useful framework for thinking about CMD, the need to perform both invasive and noninvasive characterisation may be one of the factors that have led to the poor uptake of this in routine clinical practice. Rahman et al. have shown that in patients with a high pretest probability of coronary vascular abnormality, that is, convincing history and presence of cardiovascular risk factors, CFR < 2.5 reliably identifies patients with NOCAD who will have myocardial ischaemia on CMR imaging (82% with CFR < 2.5 had stress perfusion defects vs. 22% with CFR ≥ 2.5) [5,6]. Therefore, we believe that a definite diagnosis of CMD can be achieved using a single invasive test that involves physiological assessment of the coronary vasculature. Equally, in patients who have a CT coronary angiogram as the initial investigation for angina, it may prove possible to make a diagnosis of CMD with a high degree of certainty on the basis of a high resolution stress perfusion CMR alone, without recourse to an invasive assessment. However, this assertion needs to be evaluated further and it should be noted that, at present, there is no noninvasive test for VSA.
Patient outcomes
Patients with angina and NOCAD have a poor quality of life, with 44% of patients continuing to suffer from chest pain after 12 months from their diagnosis of NOCAD [18]. These patients score similarly on the Seattle Angina Questionnaire (SAQ), for both physical limitations and quality of life, as patients with obstructive CAD [18]. They are also more likely to suffer from depression and anxiety either concurrently or as a result of their persistent symptoms [19], and they are more likely to utilise the healthcare system than patients with obstructive CAD [19].
There has been much debate over the long-term outcomes of patients with CMD. Earlier studies had shown that patients with cardiac syndrome X (CSX) had a favourable long-term prognosis [20]. CSX is an umbrella term that was previously used to describe patients with angina with NOCAD, and it comprised of several pathologically distinct diagnoses. Recent studies; however, have consistently reported adverse outcomes in patients with confirmed CMD. Of note, AlBadri et al. have reported that CFR < 2.3 independently predicted a higher risk of composite endpoint of death, myocardial infarction (MI), stroke and hospitalisation for heart failure in women with NOCAD and nonendothelium dependent microvascular dysfunction at a median follow-up of 9.7 years [21]. They also reported a trend towards higher rates of the composite endpoint in women with endothelium-dependent dysfunction [21]. Pepine et al., similarly, showed an increase in the composite outcome of death, nonfatal MI, nonfatal stroke, or hospitalisation for heart failure in women with NOCAD and CFR < 2.32 [22]. Murthy et al. reported an increased incidence of MACE, defined as cardiac death, nonfatal MI, late revascularisation and hospitalisation for heart failure, in patients with NOCAD and CFR < 2.0 on PET imaging after a median follow-up of 1.3 years [23]. CFR was a powerful predictor of MACE in their patient cohort [23]. Suwaidi et al. assessed endothelium-dependent microvascular function in 157 patients with angina and NOCAD [24]. Over a 28-month mean follow-up, none of their patients with normal endothelial function or mild endothelial dysfunction (0–50% increase in CBF in response to intracoronary acetylcholine) suffered from any adverse events. However, 14% of patients with severe endothelial dysfunction (<0% increase in CBF) suffered from MACE, which included MI, future revascularisation or cardiac death [24].
Although the overall survival is reported to be good in patients with VSA, Takagi et al. reported a MACE rate of nearly 6%, comprising death, nonfatal MI, unstable angina, heart failure or appropriate implantable cardioverter defibrillator shocks in their cohort of 1429 patients (median follow-up of 32 months) [25]. Sato et al., similarly, reported a MACE rate of approximately 5% during a mean follow-up of 49 months in 873 patients with VSA [26].
The impact of metabolic and chronic inflammatory disorders on coronary microvascular function
Diabetes mellitus has long been linked with coronary microvascular dysfunction. A recent study has reported that 72% of patients with angina, NOCAD and diabetes mellitus have CMD [27]. This study also reported an association between glycated haemoglobin (HbA1c) levels and endothelial-independent and endothelial-dependent coronary microvascular function in patients with diabetes mellitus. These findings suggest a link between glycaemic control and coronary microvascular dysfunction, and may implicate CMD as a potential mediator of ischaemia in patients with diabetes mellitus [27].
Along with diabetes mellitus, CMD has also been shown to be prevalent in patients with chronic inflammation, such as in inflammatory rheumatological disorders [30]. In the early stages of inflammatory rheumatological disorders pro-inflammatory mediators, such as tumour necrosis factor-alpha, promote endothelial dysfunction by reducing the synthesis and bioavailability of NO through a reduction in the expression of eNOS. Inflammatory cytokines are also responsible for the increased production of reactive oxygen species, which contribute to limiting NO availability [30].
Assessment of the coronary microvasculature
The coronary microvasculature cannot be directly visualised but there are several techniques to assess coronary microvascular function. In patients with NOCAD, CFR is the most commonly used test of microvascular function. Coronary microvascular function can also be assessed noninvasively, primarily using techniques that estimate myocardial perfusion at rest and during stress. In the following section, the practical aspects of making these assessments are discussed as well as their advantages and disadvantages.
Invasive intracoronary assessment in the catheter laboratory
Invasive intracoronary microvascular assessment is well tolerated and provides an accurate and reproducible evaluation of microvascular function [31]. The 2019 ESC guidelines recommend intracoronary microvascular assessment in patients with angina and NOCAD (class IIa recommendation) [32]. Invasive CFR requires measurement of coronary flow. While absolute coronary flow is difficult to measure in a clinical setting, it can currently be estimated by one of two techniques: Doppler to measure coronary flow velocity or thermodilution to measure cold bolus transit time, each requiring the use of different sensor-tipped ultra-thin intracoronary guidewires. CBF is estimated at rest and in response to adenosine (to test nonendothelium dependent function) or acetylcholine (to test endothelium-dependent function). In the absence of epicardial obstructive CAD, an impaired CFR (defined as <2.5 or <2.0 depending on the outcome measure) diagnoses the presence of CMD [33].
In patients with symptoms consistent with VSA, it is diagnosed by demonstration of either transient ischaemic ECG changes during a spontaneous episode or epicardial coronary vasospasm (>90% reduction in epicardial coronary artery diameter) associated with ECG ischaemic changes and chest pain in response to a provocative agent [35]. However, the test only has modest sensitivity (approximately 70%), especially in younger patients. Furthermore, female patients are more likely to be hypersensitive to acetylcholine provocation, giving rise to false positives [36]. However, it should be noted that there are several logistical difficulties with carrying out acetylcholine-based endothelial function testing and its availability is currently restricted to specialist centres, although this is likely to increase following recent demonstrations of its utility. In view of this, the authors recently published a stepwise diagnostic algorithm that can be used in any patient with angina who presents to the cardiac catheter laboratory [37].
Noninvasive assessment of the coronary microvasculature
start here.